Eyes
Babies can see from birth. Their vision isn’t developed completely though. The fine detail that will be achieved later is missing. Babies can distinguish bright colors well and are good at dark and light contrasts.
Babies can see small objects as early as 3 to 4 months. They can distinguish between some colors well, especially reds and greens. They can decide if a face is real or drawn.
Vision screening Vision screening starts with the my first visit in the hospital with your baby. Some babies were born prematurely or required prolonged periods of oxygen. I recommend an eye specialist for a detailed exam.
Vision screening starts with the my first visit in the hospital with your baby. Some babies were born prematurely or required prolonged periods of oxygen. I recommend an eye specialist for a detailed exam.
I check the alignment of babies eyes during the following six months.
By the age of 3 or 4 eyes are examined more closely and any history of problems is evaluated.
At the age of five a thorough eye screening is necessary. I am able to pick up problems with visual acuity screening and check for diseases of the eye.
Many infants appear to have eyes that appear crossed when they are not. This false crossing is caused by the normal widened bridge of the nose. Most children lose the appearance of the crossed-eyes as they grow.
Four out of every 100 children will have one or both eyes that are misaligned. One eye will look forward while the other turns inward, outward, upward, or downward. Some children are born with eye muscles that need lengthening or are too tight. Surgery is required to correct the problem. Other children have a problem with farsightedness and this causes their eyes to turn off at a incorrect angle. This can be corrected with glasses. Because children may compensate for poor vision in one eye, they turn off the vision in the weaker eye and this leads to Amblyopia (lazy eye) or loss of depth perception. In some rare situations a cataract or eye tumor can cause an eye to turn out of alignment.
At 4 months their eyes work in a fine, coordinated manner and have some depth perception.
Older children might give different cues to their eye difficulties. If their eyes seem to be miss aligned crossing or straying outward or inward, you should call for an appointment to confirm the problem and get directed for consultation. This is a common problem and is usually corrected with glasses, but it can indicate other medical conditions.
Some children are noticed to have a white pupil. This can indicate anything from a cataract to a tumor of the eye. It requires your immediate attention and a call for a eye exam.
Other children can complain of eye pain or redness of the eye. This can be caused by a minor eye infection like pink eye or a more serious disease of the eye. I can usually determine the cause after a brief visit.
Your baby is not making eye contact between 2 to 3 months. Constant eye crossing or one eye that turns outward is probably abnormal. Babies over 3 months of age should be able to follow a moving object. You can test this by moving a brightly colored toy in front of their eyes, although you should avoid distracting them with your voice so you can get an accurate idea.
These are warning signs of eye problems that you could notice at any age:
- Your child’s eyes flutter up and down or side to side.
- The eyes are always watery.
- The eyes are always sensitive to the light.
- Any change in the eye from their normal appearance
- If you see white, yellow-white, or grayish-white material in the pupil
- There is redness in either eye that does not go away in a couple of days
- There is continued pus or crust in either eye
- The eyes are crossed, turn out or don’t focus
- Your child often squints
- Your child often tilts or turns his or her head
- The eyelids appear to droop
- The eye appears to bulge
 Amblyopia is reduced vision in one eye because of lack of use. It occurs in one eye only. Any condition that interferes with normal vision can hinder the development of vision and result in amblyopia. About 2% of children are affected by Amblyopia. Some of the causes of Amblyopia are strabismus (eyes misaligned), droopy eyelids or ptosis, cataracts (clouding of the lens of the eye), or refractive errors. Early treatment will provide the best outcome, but vision lost from amblyopia will not return to normal.
Amblyopia is reduced vision in one eye because of lack of use. It occurs in one eye only. Any condition that interferes with normal vision can hinder the development of vision and result in amblyopia. About 2% of children are affected by Amblyopia. Some of the causes of Amblyopia are strabismus (eyes misaligned), droopy eyelids or ptosis, cataracts (clouding of the lens of the eye), or refractive errors. Early treatment will provide the best outcome, but vision lost from amblyopia will not return to normal.
Cataracts are damaged lens of the eye. They are clouded and prevent the normal amount of light from penetrating to the retina. Cataracts can appear at birth or any time afterward. Injury can cause the formation of a cataract. Early detection of cataracts is essential to allow the normal development of vision. The exam for cataracts is a critical part of the first few baby exams. It is very important to discover them early to allow the best chance for good vision. Cataracts are not common in infancy or childhood and there is no relationship to the cataracts found in older age groups.
Glaucoma is a condition where pressure inside the eye rises too high. Glaucoma can cause total blindness and requires early treatment. Warning signs include tearing, eye pain, and sensitivity to light. You might notice spasms of the eyelids, an enlarged eye or cloudy cornea. Glaucoma usually requires surgery to prevent blindness.
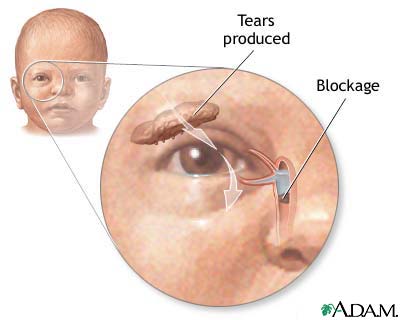 The tear duct system is an important part of the eye’s protective mechanism.
The tear duct system is an important part of the eye’s protective mechanism.
It starts functioning fully within the first few months of life. For some infants, the process of opening is delayed up to 9 months. You might notice increased tearing in one or both eyes. Sometimes this excessive tearing can be a result of other medical conditions like glaucoma. If you notice continued tearing you should call the office for an appointment. You can try gentile massage near the eye to open the tear duct. I can show you a massage technique in the office. If massage and a reasonable waiting period are not followed by normal tearing, probing the tear duct could be necessary. Unfortunately, there is not much scientific evidence that the massage is producing beneficial results.If necessary, I can refer you to the eye surgeon who will do the probing procedure.
Farsightedness or hyperopia is normal in most infants and children Mild degrees do not require correction and only should be monitored if the eyes are crossing or visual difficulties become excessive. This condition can be corrected with corrective glasses.
Astigmatism is a condition where the cornea is irregularly shaped.
It can cause blurring of vision and might require glasses for correction.
children and makes it difficult to see objects clearly when they are far away. This condition is rare in infants and toddlers, but is much more common as children approach school age. Eyes can correct the vision problem but they will not cure the condition. The condition will usually progress through the teen-years, so I recommend yearly vision screening. I am able to pick up the risk for nearsightedness in the office and will refer you to an optometrist or ophthalmologist for corrective lens if needed. the white part of the eye. You will notice excessive tearing, a pussy discharge, a feeling of something in the eye, or itching. Blepharitis is usually treated with warm compresses. If an infection develops antibiotics might be necessary. If you notice this condition you should call the office for an exam.
 Ptosis or drooping eyelids is a description of eyelids that don’t open completely. This is caused by muscle weakness in the eyelids. If there is a mild degree of weakness no serious problems occur and no treatment is required. In some situations the weakness is so severe it interferes with normal vision. If the ptosis is present in infancy, it is essential that it is corrected promptly so that normal vision develops. When the weakness is severe, surgery is required to repair it.
Ptosis or drooping eyelids is a description of eyelids that don’t open completely. This is caused by muscle weakness in the eyelids. If there is a mild degree of weakness no serious problems occur and no treatment is required. In some situations the weakness is so severe it interferes with normal vision. If the ptosis is present in infancy, it is essential that it is corrected promptly so that normal vision develops. When the weakness is severe, surgery is required to repair it.
Swollen eyelids or blepharitis is an inflammation in the oil glands of the eyelid. You will notice swollen eyelids and crusting of the eyelashes . This is most common in the morning. The eyelids might also be tender and cause a feeling of something in the eye. Blepharitis is usually treated with warm compresses. If an infection develops antibiotics might be necessary. If you notice this condition you should call the office for an exam.
 Conjunctivitis or “pink eye” will be noticed as a reddening in the white part of the eye. You will notice excessive tearing, a pussy discharge, a feeling of something in the eye, or itching. Conjunctivitis can happen at any age and at any time of the year. For most children it is caused by a viral or bacterial infection. It can also be caused by an allergy or an irritation from chemicals or smoke. Depending on the cause of conjunctivitis I might treat the eye with eye drops or ointment. Ususally eye discharge that is yellow or green are most likely to be helped by antibiotics. Good hand washing helps prevent the spread of the infection to other members of the family or friends. If the conjunctivitis is in a preteen or teenage girl and eye makeup is used, consider the makeup contaminated and toss it away and don’t restart makeup until the infection is gone – about five days. If there are questions about whether there is conjunctivitis we will make an appointment to see your child or refer you to an after hours clinic if it is a weekend or night time need.
Conjunctivitis or “pink eye” will be noticed as a reddening in the white part of the eye. You will notice excessive tearing, a pussy discharge, a feeling of something in the eye, or itching. Conjunctivitis can happen at any age and at any time of the year. For most children it is caused by a viral or bacterial infection. It can also be caused by an allergy or an irritation from chemicals or smoke. Depending on the cause of conjunctivitis I might treat the eye with eye drops or ointment. Ususally eye discharge that is yellow or green are most likely to be helped by antibiotics. Good hand washing helps prevent the spread of the infection to other members of the family or friends. If the conjunctivitis is in a preteen or teenage girl and eye makeup is used, consider the makeup contaminated and toss it away and don’t restart makeup until the infection is gone – about five days. If there are questions about whether there is conjunctivitis we will make an appointment to see your child or refer you to an after hours clinic if it is a weekend or night time need.
Your baby is not making eye contact between 2 to 3 months. Constant eye crossing or one eye that turns outward is probably abnormal. Babies over 3 months of age should be able to follow a moving object. You can test this by moving a brightly colored toy in front of their eyes, although you should avoid distracting them with your voice so you can get an accurate idea
Styes
 Styes are infections of the glands along edges of the lids of the eye. These small abscesses appear like red, tender bumps. They grow quickly and within a few hours or a day, they are full size.
Styes are infections of the glands along edges of the lids of the eye. These small abscesses appear like red, tender bumps. They grow quickly and within a few hours or a day, they are full size.
 Chalazion is a condition commonly confused with a sty. It is a bump within the lid not usually along its edge and grows slowly over weeks or months. A Chalazion is a fluid filled cyst. Styes are a bacterial infection and a chalazion is probably the result of an irritation or defect in the lid. Chalazions are treated and removed by an eye surgeon. While I can advise you how to treat a sty, if you aren’t sure which your has, you can treat it as a sty without harming the eye.
Chalazion is a condition commonly confused with a sty. It is a bump within the lid not usually along its edge and grows slowly over weeks or months. A Chalazion is a fluid filled cyst. Styes are a bacterial infection and a chalazion is probably the result of an irritation or defect in the lid. Chalazions are treated and removed by an eye surgeon. While I can advise you how to treat a sty, if you aren’t sure which your has, you can treat it as a sty without harming the eye.
Treat styes by applying warm compresses for 5 to 10 minutes 3 or 4 times a day. The warmth allows the infection to form a tip which will drain. The drainage does not usually require any antibiotics. Antibiotics will be of little benefit in most situations. If the sty does not improve after a couple of days, call my office for an appointment so I can determine the nature of the condition.
Your child’s eyes need to be clean and protected from fine materials that may lodge in them. In infancy, the natural drain for tears may not be well developed or it may even be totally blocked. In most cases, you will clearly see tears flowing from one or both eyes without any obvious cause. In time this blockage will open without any special treatment.
In the past I recommended a circular massage, applying even pressure at the space between the bridge of the nose and the inner corner of the eye. The massage lasts for about a minute, four times a day. Within weeks the tearing decreases or disappears. Some believe there is little benefit from the massage, but I have not seen any harm from this simple action.
Some children develop secondary eye infections without any obvious cause or following a common cold or sinus infection. These infections often require antibiotic drops and this is done at the office visit. If there is no improvement by six to 9 months of age, I recommend a second opinion from an eye specialist. The ophthalmologist will determine if surgical probing is necessary to open the blocked tear or lacrimal duct.